The Science Behind Intermittent Fasting for Weight Management and Health Outcomes
I started studying intermittent fasting because I really want to look at diets that people can actually do. I don’t think intermittent fasting is better than anything else – I think it’s just another tool in our toolbox to use for people that are sick of counting calories, macros or other things. It definitely seems to work.” – Dr. Krista Varady
Intermittent fasting (IF) diets are rising in popularity and more human clinical trials are being conducted to determine their safety and efficacy. The most studied forms of intermittent fasting to date include alternate day fasting (‘fast day’ alternating with ‘feast days’), the 5:2 diet (two fast days and five feast days per week), and time-restricted eating (only eating within a specific window of time each day). However, only a few studies have examined the health benefits of these diets in humans. This episode discusses these findings and shares insights into the effects of intermittent fasting on body weight and risk factors for cardiometabolic disease as well as practical advice for how to incorporate intermittent fasting diets and recommendations for future research.
Tune into this episode with IF researcher Dr. Varady to learn about:
Different types of IF and why it’s rising in popularity
How much research has been done in animals and humans
What the research shows regarding safety and efficacy
How IF may impact cardiometabolic risk factors including blood pressure, lipids, glucose, insulin, insulin resistance, inflammation and oxidative stress
What IF research has shown regarding diet quality and protein intake
Whether fasting has been shown to trigger overeating
The role of behavior change counseling
What the research indicates about maintenance of lean body mass and maintaining weight loss
Potential adverse effects of IF
Limitations in the research
How post-menopausal women respond to IF
A new study on IF and type 2 diabetes
An overview of what the body of research shows regarding breakfast and weight management
Future research directions for IF
Tips for getting started, who might benefit most and who may not be a good candidate
Krista Varady, PhD
Krista Varady, PhD, is a Professor of Nutrition at the University of Illinois, Chicago. Her research focuses on the efficacy of intermittent fasting for weight management and metabolic disease risk reduction in adults with obesity. She has been studying fasting for almost 20 years and is one of the top researchers in this field. Her work is funded by the NIH, American Heart Association, and the University of Illinois. She has published over 100 publications on this topic, and is also the author of a book for the general public, entitled The Every Other Day Diet.
[00:00:00] Voice Over: Welcome to Sound Bites, hosted by registered dietitian nutritionist, Melissa Joy Dobbins. Let’s delve into the science, the psychology, and the strategies behind good food and nutrition.
[music]
[00:00:24] Melissa Joy Dobbins: Hello and welcome to the Sound Bites podcast. Today’s episode is about the safety and efficacy of intermittent fasting in humans. What does the research show? My guest today is Dr. Krista Varady. She’s a professor of nutrition at the University of Illinois, Chicago. Her research focuses on the efficacy of intermittent fasting for weight management and metabolic disease risk reduction in adults with obesity.
She has been studying fasting for almost 20 years and is one of the top researchers in this field. Her work is funded by the NIH, the American Heart Association, and the University of Illinois. She has published over 100 publications on this topic and is also the author of a book for the general public titled The Every Other Day Diet. Welcome to the show, Dr. Varady.
[00:01:14] Krista Varady: Thanks so much for having me.
[00:01:16] Melissa: We have a lot to dig into, a lot of questions for you, but I want our listeners to know that this episode is not sponsored. I would love to hear a little bit more about your background. I would love for our listeners to learn more about your education, the work you do. I’m curious how you got interested in this topic.
[00:01:33] Krista: Oh, sure. All of my education has been in human nutrition research. I did my bachelor’s degree at University of Guelph in Canada in dietetics. I didn’t get my full RD though. I didn’t end up doing the internship. Instead, I transitioned into a PhD at McGill University in Montreal. That’s where I first got involved in clinical trials of nutrition. Then I ended up doing a postdoc at UC Berkeley to look more at calories restriction and intermittent fasting diets.
[00:02:06] Melissa: Great. What got you interested in the field of nutrition to begin with?
[00:02:10] Krista: I was an athlete in high school and I definitely noticed that when I ate better right before working out, I would do a lot better, just performance-wise. I thought there was a really cool link there. That’s what got me started into it.
[00:02:24] Melissa: Interesting. Let’s start with some definitions. There’s intermittent fasting itself. Then there’s some other terms that I would love for you to explain because we’ll be using those moving forward.
[00:02:34] Krista: Sure. Intermittent fasting is an umbrella term for basically two major types of diets. The first one is called ‘alternate-day fasting.’ That’s when people can basically have a feast day alternated with a fast day. On the fast day, you can either do no calories at all. Just water all day or most people end up having a small meal on the fast day of about 500 or 600 calories, usually as a lunch or a dinner. Then that fast day is alternated with a feast day where people can eat whatever they want. The diet flip flops like that, like feast day, fast day, feast day, fast day, indefinitely.
That one’s not so popular anymore. I started studying intermittent fasting looking exclusively at alternate-day fasting, but time-restricted eating is the other major form and that is definitely way more popular. That one involves eating within a certain window of time each day. Usually about four hours as the shortest eating window all the way up to about 10 hours per day. You can place that window wherever you want in the day. that’s like the easier way to do intermittent fasting.
That also involves like fasting a little bit every day because during the fasting period, you basically consume just water or energy-free drinks. Then the coolest part about that diet is that during the eating window, say if you pick an eight-hour eating window, you don’t have to count calories at all or count carbs or anything like that. It’s just a really simple diet where you eat within a certain window of time that you pick and then fast with water for the rest of the day.
[00:04:12] Melissa: Great. We’re going to dig into the research on this. How much research, animals versus humans, and then the different types of intermittent fasting or time-restricted eating. We have a really good review article to share with the listeners as well, whether you’re a health professional or just the lay public. I think it’s a really great overview. Krista, you were the lead author on that. I found that very helpful in preparing for this interview. Why do you think– You teased it already. We don’t have to count stuff. That’s huge. Why do you think that intermittent fasting or time-restricted eating is rising in popularity?
[00:04:51] Krista: I think people just got really burnt out of all the previous main or fad diets. In the ’80s, we were really obsessed with low-fat diets. Then in the ’90s, 2000, it all became about Atkins and carb counting. Then, calorie restriction where we’re counting calories has always been pretty big. All the previous diets really focused on heavily monitoring macros and energy. I think people are just sick of it.
With time-restricted eating, you really just have to, you start eating, let’s say, at 12:00 PM. Don’t count calories. Do whatever you want until 8:00 PM. Try to focus on healthy foods, but you don’t have to monitor anything specifically. Then after 8:00 PM, you just fast with water until noon the next day. It’s just simple. I think the simplicity and just how different it is from previous diets is what has made it really popular.
[00:05:46] Melissa: Talk to me about how much research has been done in this area. In the intro, I explained that you’re one of the top researchers in this field. Talk to me about how much research has been done, animals versus humans and just the breadth of knowledge that we have so far.
[00:06:02] Krista: Oh, sure. We started looking at intermittent fasting in humans maybe about 15 years ago, but there was very few studies in humans up until about five years ago. Then it exploded on the scene. Now, there’s probably a new study published for time-restricted eating, specifically. There’s probably one every week, honestly. There’s been a tremendous amount of scientific interest in it. I think that follows what the general public’s doing. We’re noticing that people are incorporating this into their lifestyle and they seem to like it. I think the science is following that.
Before that, there were a lot of animal studies, but I hesitate to comment on the animal studies because I find that a lot of what we see in animals is just not being reproduced in humans. Fasting a mouse for a day, it’s like fasting a human for a week. You get like really amazing findings in animals and then none of that’s really being reproduced in humans because people, they do the diet, but they don’t adhere to it perfectly. Then, also, the fasting period is just not that long in humans. We’re not getting these crazy effects that you’d see in mouse models.
[00:07:13] Melissa: Interesting. I know we might continue to touch on that as we go through this conversation. What does the current research show overall? I’d love to hear about safety, efficacy, benefits. This review article has a nice summary of the different studies, length of studies, population studies. I know I’m throwing a lot at you, but tell us about where the research is at right now.
[00:07:39] Krista: Sure. Starting with population studies, we definitely find that people are doing time-restricted eating a lot more than alternate-day fasting. They just find it easier to do and people can stick to time-restricted eating pretty well. Most of the research shows that people will stick to that eight-hour window on generally six out of seven days per week. If they don’t stick to it, it’s usually like a weekend day, like a Saturday, just because that’s when a lot of social eating events occur.
[00:08:09] Melissa: Life happens.
[00:08:10] Krista: Yes, exactly. We know that people aren’t perfect, so that’s fine. It’s that whole thing with what dieticians say like everything in moderation. I really believe in that or hopefully, they’re still saying that. I don’t know.
[00:08:21] Melissa: Yes.
[00:08:23] Krista: Some do, yes.
[00:08:25] Melissa: Meet people where they are, right?
[00:08:27] Krista: Yes, exactly. Then just to step back a bit, I started studying this because I really want to look at diets that people can actually do. I don’t think intermittent fasting is better than anything else. I think it’s just another tool in our toolbox to use for people that are sick of calorie counting or sick of doing other things. It definitely seems to work. Specifically the main effect we’re noticing is weight loss. People will lose anywhere from about 3% to 5% of their body weight. A lot of that weight loss will peak around three to six months. With any dietary intervention, people can do it for about three to six months really well. Then after that, they enter more of a weight maintenance phase.
We also noticed some cardiometabolic benefits. Blood pressure has been shown to go down by about 5 or 10 points, primarily systolic blood pressure. Plasma lipids don’t really get affected. There has been the occasional study that shows that LDL cholesterol and triglycerides go down, but in general, we’re not really seeing much of an effect there. I think it’s just because a lot of people– We study people with obesity and a lot of these people are, if they do have high cholesterol, they’re already on medications for that. Most of the people that enroll in these studies already have normal cholesterol levels. It’s really hard to see changes in cholesterol if somebody is already in the healthy range.
The other part, other than just weight loss, the main benefit is really in glycemic
control. We’re noticing that intermittent fasting helps reduce fasting insulin levels and then it also reduces insulin resistance in people that have obesity and then pre-diabetes. Then, I think you’ll probably ask a question about the type 2 diabetes study we did. I can talk about that population group in a second.
[00:10:21] Melissa: Yes, absolutely.
[00:10:22] Krista: Just to summarize, weight loss for sure, maybe a bit of blood pressure lowering and definitely improvements in blood sugar regulation.
[00:10:31] Melissa: Great. Safety considerations, anything to point out there?
[00:10:37] Krista: A couple of the major questions I get are, does it cause eating disorders if you’re intermittent fasting? Which is a very valid concern. We’ve shown in our studies– First of all, we exclude people that have a history of eating disorders. I don’t think that fasting is really good for that population group. In people that do not have a history of eating disorders, it doesn’t increase eating disorder behaviors. We measure this using questionnaires. That’s one safety issue.
In general, in terms of adverse events, the main thing that people report are headaches and that’s usually just in the first week or so of the diet. That usually occurs because of dehydration. They’re dehydration-induced headaches. When people drink enough water or just up their water intake during the eating period and fasting period, those headaches tend to go away.
Then, another misconception is that fasting will tank someone’s metabolism. By this, I think they’re talking about like resting metabolic rate. Just to point out that whenever somebody loses weight, I know it’s a lot of dietitians and health professionals listening to this, your resting metabolic rate is very strongly determined by how much muscle mass you have. Then whenever somebody loses weight, most of it is fat mass, about 75% typically. Then about 25% will be lean mass of that total weight loss. Then when that lean mass goes down, that lowers resting metabolic rate a little bit too. About 100 calories or so per day.
That happens because of the weight loss and not the fasting per se. We see the same thing in just daily calorie restriction studies as well. It doesn’t mess with your metabolism or change that any more than a typical weight loss diet would.
[00:12:26] Melissa: In all of your research that you’ve been doing, talk to me about the length of the studies and maybe some of the goals or limitations with that, working with real people, randomized control trials.
[00:12:36] Krista: That’s right. We’re probably always running two or three randomized control trials. We’ve run studies that are as short as two months, but now we’re really focusing on longer-term studies, six months or twelve months because those are the studies that help make medical decisions and those can help change clinical guidelines. Potentially, intermittent fasting can be incorporated into guidelines more so than they are now. That’s the main thing we do. I run exclusively human studies, just to clarify that.
[00:13:06] Melissa: Again, we can talk more about that as it’s warranted, but the differences you noted between animals and humans, and I know that’s the case across all nutrition research, but it seems like in particular with this topic that those results in animal trials aren’t really applicable in humans for a lot of reasons.
[00:13:26] Krista: We didn’t know this about 10 years ago and a lot of the news would pick up on these animal studies and say, “Wow, diabetes has been reversed and these animals are losing 30% of their body weight.” It was just these incredible findings. I think the general public will now see a lot of the human evidence that’s now coming out and be frustrated thinking, “Oh, I thought I was going to lose a ton of weight,” or, “I thought my diabetes was going to be a reverse.” Whereas now, that we actually have human data, we find that sure, it is working, but it’s not as an amazing of an effect.
We’re not reversing type 2 diabetes. We’re lowering A1C and lowering medication use, but we’re definitely not seeing anything that we would in the animal models. Just to get into this in a bit more detail. A mouse will achieve full-blown ketosis in 24 hours, whereas in humans, that can take anywhere from three to eight days. Their resting metabolic rate is extremely high per kilogram of body weight. If you don’t feed a mouse in four days, it will die. Whereas, with humans, depending on how much fat stores we have, we could last for months. Then, they’re nocturnal.
They’re just not good specimens for this. Sure, if you want to run maybe some complicated mechanistic studies, fine. I’m just sick of seeing these mouse studies come out and people wondering why they’re not translating it to humans. Honestly, I just don’t think they’re good models for any efficacy or safety studies.
[00:14:56] Melissa: Thank you. Let’s talk about diet quality and protein intake, maybe the protein first. We’re talking about the loss of lean body mass anytime you restrict calories and lose weight that is no different with intermittent fasting or time-restricted eating versus other types of diets. Has your research looked at if there’s adequate protein intake during that feasting window? Does that mitigate some of this lean body mass? Do you have any data or results that you can share regarding that?
[00:15:30] Krista: Oh, yes, for sure. We haven’t run those studies. There’s a researcher named Grant Tinsley, who looks at how protein intake combined with resistance training can help people, basically, not lose any lean mass during time-restricted eating. He’s shown that. I do have to say that a lot of those studies have been done in athletes. I’m not sure actually to date if there’s any studies in people with overweight or obesity.
In general, just looking at other data from calorie restriction trials, in order to alleviate any of that muscle mass loss, if you do up your protein intake, usually to 25% to 30% of your needs, and then also combine that with pretty rigorous regular resistance training, I think three to five days per week, you probably won’t lose any muscle mass. I think he asked about like protein quality. We haven’t measured that. We do look at dietary intake throughout all of our trials. We have people do seven-day food records regularly throughout the study.
Interestingly, we find that diet quality doesn’t change. We do give people a little bit of dietary counseling. We meet with them weekly over Zoom and try to teach them some basics like watch your portion sizes, try not to drink your calories, just all the very basic weight loss dietary counseling tips, eat more fruits and vegetables, whole grains, try to de-emphasize processed foods, that type of thing. Interestingly, it doesn’t change at all. People eat a little bit less, but they don’t change sugar intake, fiber, fruit, and vegetable intake, any of that, unfortunately.
[00:17:07] Melissa: It’d be interesting to see if they make some bigger shifts there. They’re just eating the same types of foods, just less because of that shorter window?
[00:17:20] Krista: Exactly, yes. We were hoping with the dietary counseling– We do have registered dietitians meet with them. We’ve run thousands of people through trials. I think it’s just really hard for people to change what they’re eating because that really relies– It also factors into what your family’s eating and what’s in your pantries at home type of things. We are getting people to eat less, but the food quality, it’s not great at baseline and it doesn’t tend to improve.
[00:17:49] Melissa: Is there anything else that you wanted to say regarding just diet quality in general with the research studies that you’ve done?
[00:17:54] Krista: We also look at beverage intake. I was a little worried that people would start drinking a lot more caffeinated beverages during the fasting window just to boost energy levels. We’re a bit worried about that affecting sleep and all that. Interesting. They don’t up their caffeine intake. There’s no changes in alcohol intake. It doesn’t affect beverages either.
[00:18:17] Melissa: Interesting. Regarding the different types, in the review article, it seemed to me that the alternate-day fasting was more effective than just the time-restricted eating. Can you speak to that?
[00:18:32] Krista: Alternate-day fasting does result in more rapid weight loss. It is a more intense form of intermittent fasting because you’re only having 500 calories every other day. Typically, we see about twice the amount of weight loss with alternate-day fasting as we do with time-restricted eating. The problem is people don’t stick to alternate-day fasting that well, for that long, because it’s just so hard to do. 500 calories every other day, you really got to alter your social schedule for that and your work schedule to accommodate that. Whereas time-restricted eating, the weight comes off slower, but people like it better.
One thing I forgot to mention is that the whole reason that time-restricted eating works is because when people confine their eating window to eight hours, they end up naturally cutting out about 300 to 500 calories per day, as shown in a bunch of different studies at this point. You get this unintentional calorie restriction that comes from just watching the clock and reducing your eating window a bit. Research has shown that we typically eat in a 12 to 14-hour window. Essentially, we’re just cutting out six hours of eating, which results in natural calorie restriction.
[00:19:44] Melissa: In your screening process, do you ask people about their habits and screen people out who perhaps maybe they’re eating more than the eight-hour window, but they’re not eating a lot of extra calories at night or they don’t have a big breakfast? Is there
anything that you screen out regarding that?
[00:20:03] Krista: We screen out people who eat within less than a 10-hour window because we don’t want people that are already doing the time-restricted eating diet. Other than that, we do exclude shift workers, just people like nurses or somebody who’s working a night shift, just because it’d be really hard for them to eat between 12:00 and 8:00, probably sleeping at some point during that time. Those are the major things.
[00:20:26] Melissa: Let’s talk about that diabetes study your team just finished. I think it’s the first randomized control trial for type 2 diabetes and intermittent fasting?
[00:20:37] Krista: It is, yes, it’s the first one. It was just published in JAMA Open last week, actually, and it looks at intermittent fasting, so time-restricted eating versus calorie restriction. It’s a control trial, so we have a control group. It ran for six months, and the main thing we wanted to see was, is time-restricted eating safe in people with type 2 diabetes? Does it help to lower A1C and body weight? We found, yes, it did. People lost about– How much was it? It was about 10 pounds over six months in the intermittent fasting group, and then about 6 pounds in the calorie restriction group.
It was one of our first trials to show that fasting actually produced greater weight loss than standard care, which I found really interesting. Then we looked at our questionnaire data and found that the reason that they stuck to time-restricted eating better than calorie restriction was just because they were so sick of being advised to do calorie restriction. I guess it’s just like the main thing in the ADA guidelines, American Diabetes Guidelines, just like, “Oh, you need to lower your calorie intake, so might as well start counting calories.”
A lot of people had failed previously with that and were really excited to try a new regimen that didn’t require careful monitoring of calories. They lost a little bit more weight. Their A1C went down by almost a full point over six months, which was pretty exciting. Then some of the individuals were able to lower medication use as well. We’re hoping to do a full-blown, 12-month study with a bigger population to see if some people can even reverse type 2 diabetes over a longer period of time with time-restricted eating.
[00:22:18] Melissa: I was going to ask you about this, and I know it’s in the review article, but this seems like a good place to address it, especially when you’re working with somebody who has type 2 diabetes and they’re on certain medications, what advice do you give them? Obviously, as they’re cutting back on their intake, maybe they’re getting less carbs, they might potentially have a low blood sugar reaction. What advice do you give them?
[00:22:42] Krista: First and foremost, we tell them to contact their endocrinologist. Depending on what meds they’re on, they’re definitely going to have to probably– If they’re on insulin and sulfonylureas, which are two things that can pretty greatly lead to hypoglycemia, those will need to be altered. Just to point out and be super clear about this. With intermittent fasting and type 2 diabetes, it’s not something that someone can just read on the internet and start. You really have to work with your doctor for this because medications will need to be altered.
When you do work with your doctor, we actually saw no serious adverse effects. We had people wear continuous glucose monitors so we could monitor hyperglycemia and hypoglycemia. We didn’t see that the rates of hypoglycemia were any different than in controls. We didn’t see major issues with glycemic regulation, which is great.
[00:23:36] Melissa: Just in general, with this research, are there limitations that– Obviously, with most research, there are some limitations and I always like addressing those. Is there anything you wanted to share with us?
[00:23:46] Krista: It is research in humans. I think the main limitation is that we don’t actually know what people are doing. We meet with them again, once a week. We touch base with them and we get their weights, which we measure using a standardized scale that we’ve given them. It’s like a Wi-Fi scale where we can get, an accurate weight. Other than that, who knows what people are doing? I feel like a lot of times, people will just tell us what we want to hear. Then the main way to know if they’re doing something is really by monitoring their weight. Their intake with food records and stuff like that. That’s just a part for the course.
[00:24:26] Melissa: Nutrition research, in general, it’s hard to connect those dots sometimes because you don’t know exactly what they’re doing.
[00:24:32] Krista: Exactly.
[00:24:33] Melissa: Because they’re people. Any indications from the research, and maybe we’ll see more on this as longer-term studies are being done, but as far as the maintenance phase, keeping the weight off, we briefly addressed the lean body mass. Do you measure body composition?
[00:24:49] Krista: We do, yes. We measure using DEXA in all of our trials. MRI is the best way to measure it, but DEXA is the second best and it’s a little faster and easier.
[00:25:00] Melissa: Are you seeing anything with regard to the maintenance, keeping the weight off?
[00:25:04] Krista: We finished a long-term 12-month study just this past summer that was published in Annals of Internal Medicine. That one compared time-restricted eating to calorie restriction in a control group. It was 12 months, but it was separated into a six-month weight loss phase, followed by a six-month weight maintenance phase. What we wanted to see was, could people do that eight-hour diet for the first six months and lose weight, and then can they transition into a 10-hour eating window to maintain the weight? We found that they could.
You can use time-restricted eating to maintain that weight loss. You basically just make your window two hours bigger. I do have to say, very importantly, and I’m sure other guests have said this, after someone loses weight, they have to continue some type of diet or some type of lifestyle modification. You can’t just go back to the way you were eating before, because obviously, you’ll just gain back all the weight. That’s super important.
[00:26:02] Melissa: That seems pretty reasonable to just extend that window a couple more hours. That seems pretty doable, not minimizing the efforts involved in weight loss, that’s for sure, weight loss maintenance. Back to the alternate-day fasting versus the time-restricted eating, have you seen or do you expect to see, with the time-restricted eating being easier to stick with, easier saying in a relative term, maybe it doesn’t have as significant results as the alternate-day fasting right away, but then if they can stick with it longer, have you seen or do you expect to see similar long-term results?
[00:26:38] Krista: With alternate-day fasting, honestly, people aren’t really researching that anymore because nobody seems to want to do it. Very few people do it, but I think there are more studies coming out with the long-term effects of time-restricted eating and then whether or not it can work for weight maintenance as well. I’m hoping that there’s going to be more long-term data. That’s the main thing we need right now.
[00:27:00] Melissa: Right, I’m just thinking out loud, if the data now and the long-term data shows that alternate-day fasting really is more effective, then that’s information that people would have and say, “Maybe I want to put my efforts more towards that versus the time-restricted eating, even though that’s easier to live with.”
[00:27:18] Krista: I think the main driver of everything is adherence. I think we just need to test things that people are actually going to do. I don’t think people are going to do alternate-day fasting for more than three to six months. When we ran studies in alternate-day fasting, we had 40%, 50% dropout rates, who were like, “I’m done.” With time-restricted eating, on the other hand, we’ve got 5% dropout rates, 10% dropout rates, and 80% to 90% of people say they’re going to stick to it after the study’s over, just because they find it easy to incorporate into their lifestyles, which is the most important thing.
[00:27:51] Melissa: Exactly, very cool. In one of your studies, you found that post-menopausal women were able to stick to the diet better than pre-menopausal women. Hopefully, I’m not saying that wrong. Could you speak to that?
[00:28:01] Krista: That’s totally correct. We’ve noticed in most of our trials of both alternate-day fasting and time-restricted eating that post-menopausal women tend to lose a bit more weight than pre-menopausal women, which is shocking because it’s always said that post-menopausal women have a harder time losing weight. We find that it’s all because they stick to the diets better. We looked into this a little bit and found that it wasn’t related to hormones or anything like that. It was just totally related to adherence. Post-menopausal women, they might have older children or children that are out of the house, so they have more time for themselves.
Having young children takes up a lot of time and it’s hard to focus or do anything for yourself when you have young kids to take care of. Then, also, I think the post-menopausal women know what works for them, so maybe they’re signing up for these intermittent fasting studies knowing that that’s something that they can do because they’ve had time to test out a bunch of different diet protocols.
[00:29:00] Melissa: I could just say from experience, the time-restricted eating window, if you’re post-menopausal and you don’t have children to worry about and feed dinner and have dinner at a certain time, you could flex your eating times a little easier for sure.
[00:29:17] Krista: Oh, definitely. That’s a really good point.
[00:29:19] Melissa: Then you didn’t think that there was anything hormonally related to the post-menopausal women being able to adhere to it, but did you monitor hormones or–
[00:29:28] Krista: We started measuring changes in sex hormones, estrogen, and testosterone, and everything in all of our studies now because I know that there was like a really– There was a rat study that came out five years ago that showed that intermittent fasting might have negative effects on reproductive hormones, but what they didn’t show was that those rats were equivalent to a nine-year-old girl. Then they said the rats didn’t hit puberty basically. I’m like, “Obviously, if you fast like a nine-year-old girl, obviously, it’s going to mess up
puberty. When we measure reproductive hormone levels in just healthy women, postmenopausal and premenopausal, we don’t really see any changes. The only time we do see changes, right now we’re running a study with women with polycystic ovarian syndrome. We find that it actually helps lower testosterone levels in those women. PCOS is basically, I guess it’s a disorder, a disease, I’m not sure what the exact term for it would be, but it’s when women make a little too much androgens and testosterone, which could lead to acne and problems with ovulation and their periods become irregular and they can also develop a bit of facial hair and just body hair.
You want to lower those testosterone levels back to the normal range. We are finding that intermittent fasting, and it might just be entirely because of the weight loss, it can help, basically, get those hormones back to where they should be. We’ll probably publish that study in about a year or so. We’re just finishing it up now.
[00:31:01] Melissa: Great. Somewhat related, there’s quite a bit of research on breakfast and weight management. I would just love for you to share your thoughts on that if you care to do that.
[00:31:14] Krista: Oh, sure. I get a lot of questions about breakfast just because with time-restricted eating, a lot of people pick the 12:00 to 8:00 window so they can still eat dinner with their families. That’s usually why they place it in the afternoon or evening. Essentially, you’re skipping breakfast while you’re doing that diet. Breakfast skipping does not result in weight gain. I know that there’s a lot out there or maybe just on social media saying that.
If you look at the studies and meta-analyses in this area, there’s a really good one if somebody wants to read it, it’s in British Medical Journal, BMJ. I think it was published two years ago. It’s a meta-analysis that just looks at all the data out there and it shows that if people skip breakfast, they don’t gain weight. It has no effect on body weight. The only effect it has on energy intake is actually potentially decreasing it by about 200 calories per day, which makes sense because you’re just skipping a meal. It doesn’t lead to being hungrier later in the day.
I think a lot of the initial breakfast-skipping studies were funded by cereal companies and they were really looking at the effect in children and looking at breakfast skipping on cognition and learning ability. Then somehow that all got transposed onto body weight and breakfast skipping. A lot of that data is not– If you look at it, the studies are poorly done.
[00:32:40] Melissa: That brings me to a question that I ask a lot of my guests who are involved in research, is the role of industry-funded research. You’ve already mentioned it a little bit, but as a researcher yourself, not all studies can be funded by the NIH. What are your thoughts on the role of industry-funded research?
[00:33:03] Krista: I think you definitely need to– Whenever I read a study or a paper, the first thing I do is I look at the funding line. Who funded it? NIH or the American Heart Association, that type of stuff. I do get a little wary when it’s funded by industry and, not to say like we have had, we’ve done a couple of different studies with Nestle and they’ve been very good. They’ve been totally hands off and they’re like, “Run the study,” and you have to really work with your IRB, like the ethics board on how much, access they’ll have to the data. We basically just don’t give them any access to anything.
We run the study and then we just publish the paper. It depends. I wouldn’t say it’s, you’re going to definitely get super bad data or not truthful data if you’re working with industry, but it’s still something you got to think about, I think because I do still find that when it is published by industry, it’s more likely to show a positive effect. Whereas when it’s funded by the NIH, I find that the findings are much more variable. It’s something to keep in mind, but industry funding doesn’t automatically mean that it’s like shady science.
[00:34:14] Melissa: A follow-up to that is, what are your thoughts on the research that just doesn’t get published? Because that, I think, is an area that there’s a lot of room for improvement is whether it showed positive, negative, neutral results is just– If it was researched is getting it published or available in some capacity.
[00:34:34] Krista: That’s changed a lot over the past 20 years. I did my PhD about 20 now. I’d say back then it was so hard to get anything published unless you showed a result, like usually a positive result, it would just get rejected. Now, that’s really changed. We published our first big study of alternate-day fasting in JAMA, Journal of American Medical Association, and we didn’t prove our hypothesis at all. We thought that people would be able to stick to alternate-day fasting better than calorie restriction because it’s just easier to do and you get a day off of dieting every other day.
That was our hypothesis. We were totally wrong. People hated the diet and dropped out. Then, JAMA still published it. It was like a null finding or a negative finding. I do find with diet studies, a lot more null effect or negative findings are being published now.
[00:35:31] Melissa: I think that’s really valuable information.
[00:35:33] Krista: Oh, absolutely. Because the other thing is, if you don’t know, it doesn’t work. If you ran a study and something doesn’t work and then it’s not published, then someone else is going to run it again and waste their money and their time on it. It’s super important to publish all findings.
[00:35:46] Melissa: Great. What have you seen in the literature about fasting mimicking diets or fasting with food?
[00:35:53] Krista: Fasting mimicking diets are like they’re considered periodic fasting, not intermittent fasting. They usually involve fasting for the first five days of every month where you use– It’s usually a really specific product set. I think it’s also very low protein. I think it’s 9% protein and it’s soups and bars and that type of thing that you can buy from these fasting mimicking companies. I’ve seen, there’s nice studies published about it, but mainly in animal models.
The research in humans shows that it works, but there are really high dropout rates because people don’t like the products themselves. Then, also, I think they have them eating about I guess 700 to 1,000 calories on those first five days of the month, but it does seem to work for weight loss. I’m always surprised though because they get these really amazing weight loss effects, similar to what we get with time-restricted eating, but they’re only doing this fasting diet for the first five days and I’m always surprised that they don’t like just eat more in the next 25 days and gain all the way back, which would be pretty easy.
I’d say we still need a lot more human data in that area to really look at those effects, but that is pretty industry-funded. Another thing to keep in mind when looking at those studies.
[00:37:15] Melissa: Thank you. Tell us your opinion on the future research directions for intermittent fasting or time-restricted eating. What do when you look into your crystal ball or what are you planning? What can you share with us?
[00:37:27] Krista: We’re running a bunch of studies now. The one on PCOS, women in PCOS, I’m starting a study, actually as we speak, in type 1 diabetes. I get a lot of questions if people at type 1 can do these diets. Before we thought that they probably shouldn’t, but now I think even in the paper that you’re about to share, it’s who probably shouldn’t do it.
I probably mentioned that type 1 should exercise caution, but we have some pilot data showing that if people basically, again, work with their endocrinologist, it is fine to basically skip breakfast. We do have to know how to change your insulin. Then you have to be wearing a continuous glucose monitor to measure hypoglycemia and hyperglycemia. That’s the major areas. We’re also thinking of running a study looking at combining those GLP-1 agonists, the weight loss drugs like Ozempic, et cetera.
[00:38:24] Melissa: Interesting.
[00:38:25] Krista: I know. Because those drugs work amazingly for weight loss, but then what we’re noticing is people are saying once they’ve reached a BMI of 25 or whenever it is, their doctors will take them off because they don’t need it anymore. Then the drugs are so expensive if you just want to stay on them yourself.
[00:38:42] Melissa: If you can get them.
[00:38:43] Krista: We want to see if people could potentially use time-restricted eating to maintain the weight loss afterwards.
[00:38:48] Melissa: Interesting. Very cool. You briefly mentioned maybe type 1 would not be a good candidate. Do you have any other insights on who might benefit most or who else might not be a good candidate?
[00:39:00] Krista: For people that shouldn’t do it, I’d say definitely not for children, people under the age of 12. There have been some studies in teenagers with severe obesity. Over the 95% for their BMI score that do benefit from it. It might be okay in teenagers. I think we still need more data there just because the risk of eating disorders in teenagers is very high.
I’d say also women who are pregnant, lactating, should probably not be doing these diets just because we have no safety data. Then also older individuals, people particularly over the age of 70, 75. We just don’t have any data on what happens to muscle mass loss and older people are at risk of sarcopenia. We need some studies before we can advise people to do it that are over 75.
[00:39:53] Melissa: Any advice for people in general or health care professionals to help their patients
and clients to get started on intermittent fasting or time-restricted eating?
[00:40:05] Krista: I’d say it’s a pretty simple diet to do if you don’t have any other diseases. First, if you have diabetes, definitely work with your endocrinologist. I think behavioral change is a really important thing as well. If people can get behavioral change counseling, I think that’s super important. Other than that, really all you do is you pick the length of your window first. Most people think eight hours and then you place it at a place in the day where that works for you that you can maintain. You don’t want to like swing the window around a lot from day to day because your circadian rhythm, it’s tough on your circadian rhythm to adjust to major swings. You don’t want to go from 8:00 AM. to 4:00 PM one day and then 12:00 to 8:00 the next day. You can wiggle it around, I’d say, by an hour or so each day. Other than that, there’s no calorie counting involved and during your fasting period, you would just stick to water and tea and coffee without additives.
[00:41:05] Melissa: Great. Thank you. I’m glad you brought up the behavior change. You do address that in this review article, which is wonderful because even though it’s a simpler, easier diet to follow, the behavior change is still a big component.
[00:41:21] Krista: Exactly. Oh, yes, behavior change, I think, is the key element to all of it. I think that’s super important thing to address.
[00:41:28] Melissa: Let’s share maybe some bottom line takeaways for our listeners as we’re wrapping up and where people can find more information about this topic. I mentioned this review article. I will have that linked in my show notes at soundbitesrd.com. You mentioned the BMJ article. Hopefully, I can get that from you and put that in the show notes as well.
[00:41:47] Krista: Oh, yes, absolutely. Then I also have an Instagram where I post research updates and just practical tips on how to do fasting. It’s at drkristavarady.
[00:41:58] Melissa: At drkristavarady on Instagram. You have quite a following and some great content that you share there. We will continue to follow you there. Is there a hub or somewhere through University of Illinois, Chicago, where you have some more of your research information or anything else we should know?
[00:42:18] Krista: Most of the research information is just on PubMed. If you want [] to look at what we’re doing, that’s where all of the papers are published and a lot of them are open access. I’d say Instagram is probably the main place to see what we’re up to.
[00:42:30] Melissa: Great. Thank you so much for coming on the show, Dr. Varady. It has been very interesting and informative.
[00:42:36] Krista: Oh, great. Thank you so much for having me. It’s been wonderful.
[00:42:38] Melissa: My pleasure. For everybody listening, if you liked this episode, please share it with a friend and come back and listen to other episodes. As always, enjoy your food with health in mind. Till next time.
[music]
[00:42:53] Voice Over: For more information, visit soundbitesrd.com. This podcast does not provide medical advice. It is for informational purposes only. Please see a registered dietitian for individualized advice. Music by Dave Burke, produced by JAG and Detroit Podcasts, copyright Sound Bites Inc., all rights reserved.
[music]
LISTEN, LEARN AND EARN
Listen to select Sound Bites Podcasts and earn free CEU credits approved by the Commission on Dietetic Registration (CDR) for registered dietitian nutritionists and dietetic technicians, registered. Get started!
Get Melissa’s Sound Science Toolkit here!
Partnerships:
Sound Bites is partnering with the Association of Diabetes Care and Education Specialists (formerly the American Association of Diabetes Educators)! Stay tuned for updates on the podcast, blog and newsletter!
Sound Bites is partnering with the International Food Information Council! Stay tuned for updates on the podcast, blog and newsletter!
Sign up for my monthly newsletter and episode eblasts so you never miss an update!
Listen on Stitcher (Android)
Install the Stitcher App
1. Search for “sound bites with melissa joy dobbins” 2. Choose Play Current Episode or Add to Playlist
Choose “Play Episode”
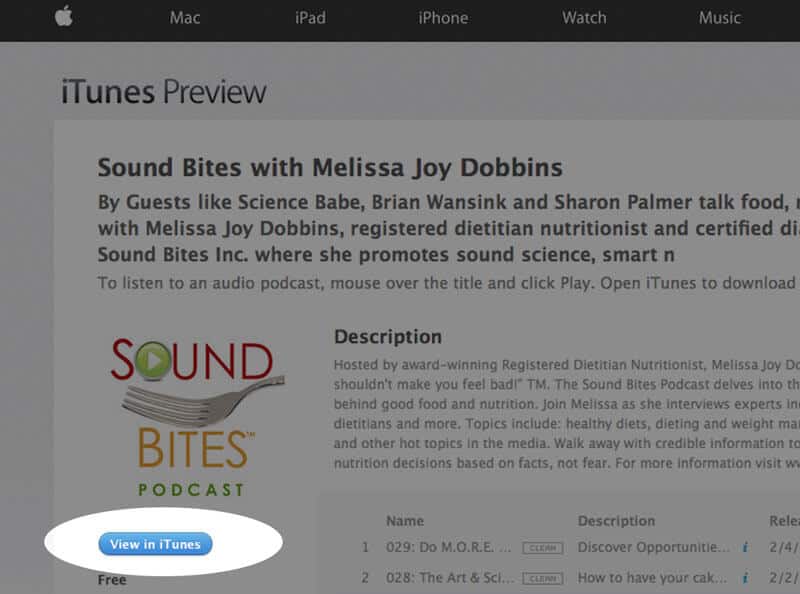
How to subscribe via iTunes
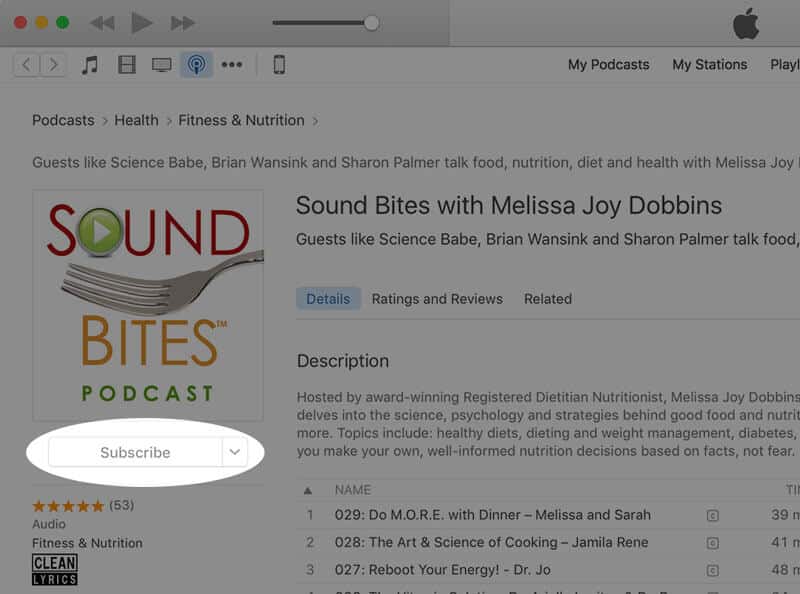
Click here to view the Sound Bites Podcastin iTunes, then click the blue “View in iTunes” button. This will open your iTunes application directly to Sound Bites Podcast. Click the “Subscribe” button, and your done!
Click “View in iTunes”
Click “Subscribe”
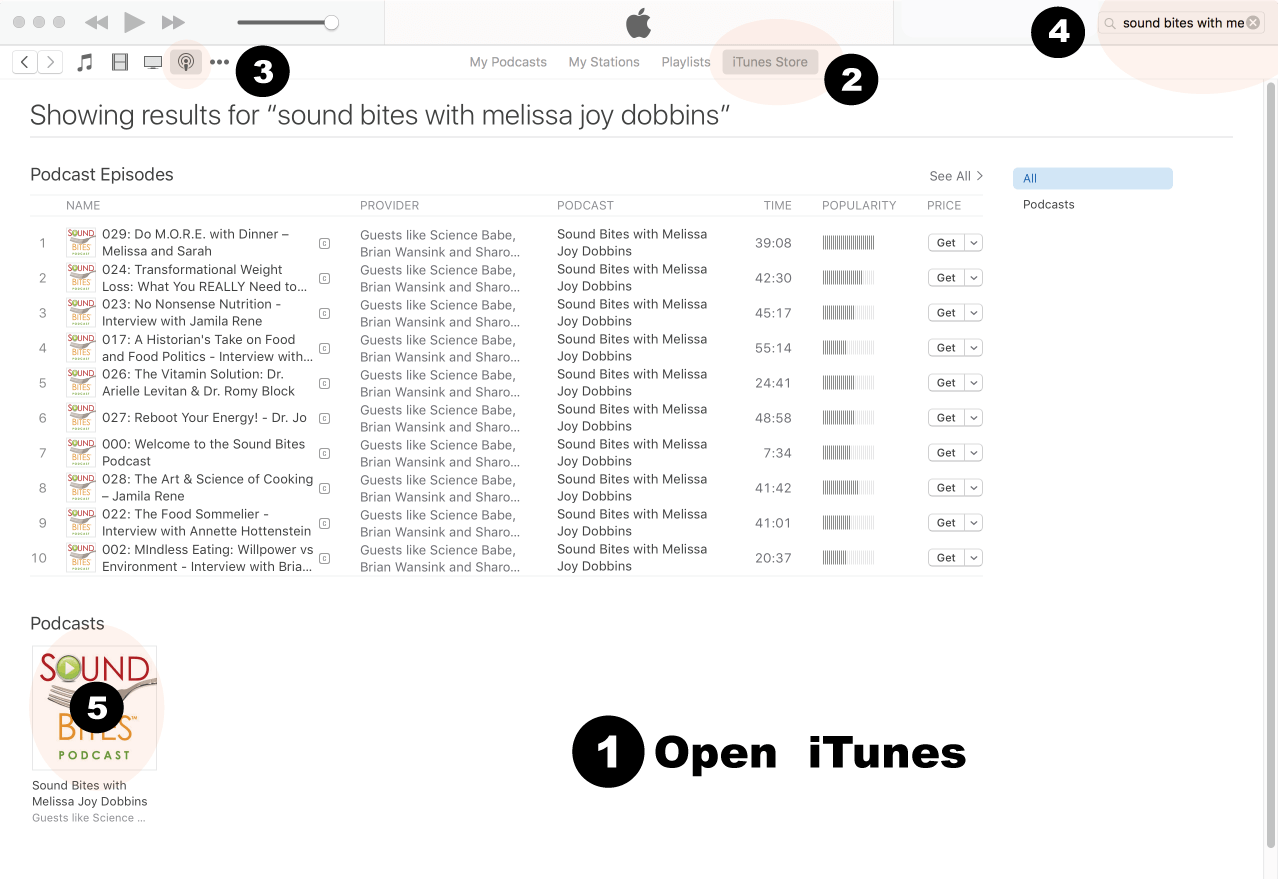
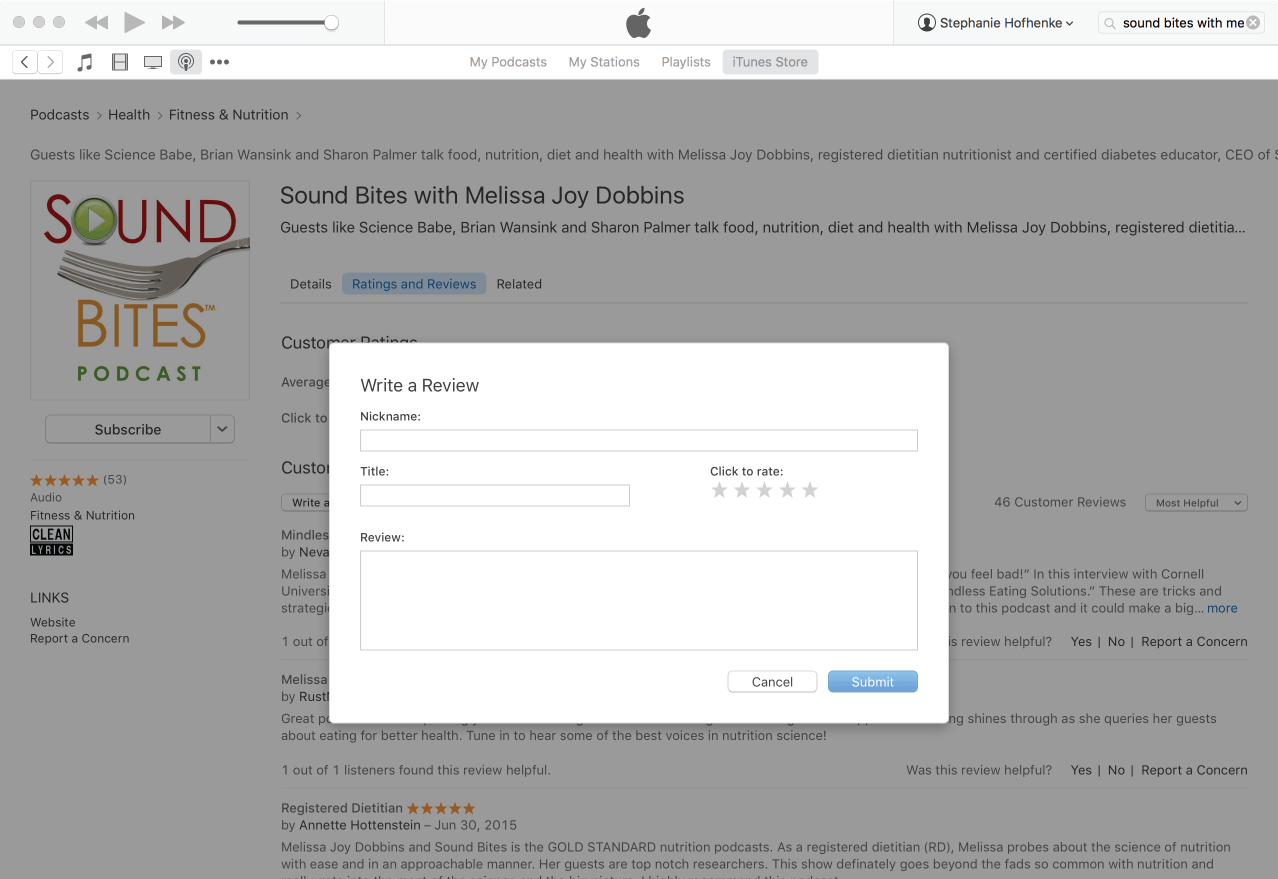
How to Review in iTunes
Open iTunes desktop application
Click iTunes Store
Click on Podcasts
Search for “Sound bites with Melissa Joy Dobbins”
Click on podcast image
Search for Sound Bites podcast in iTunes
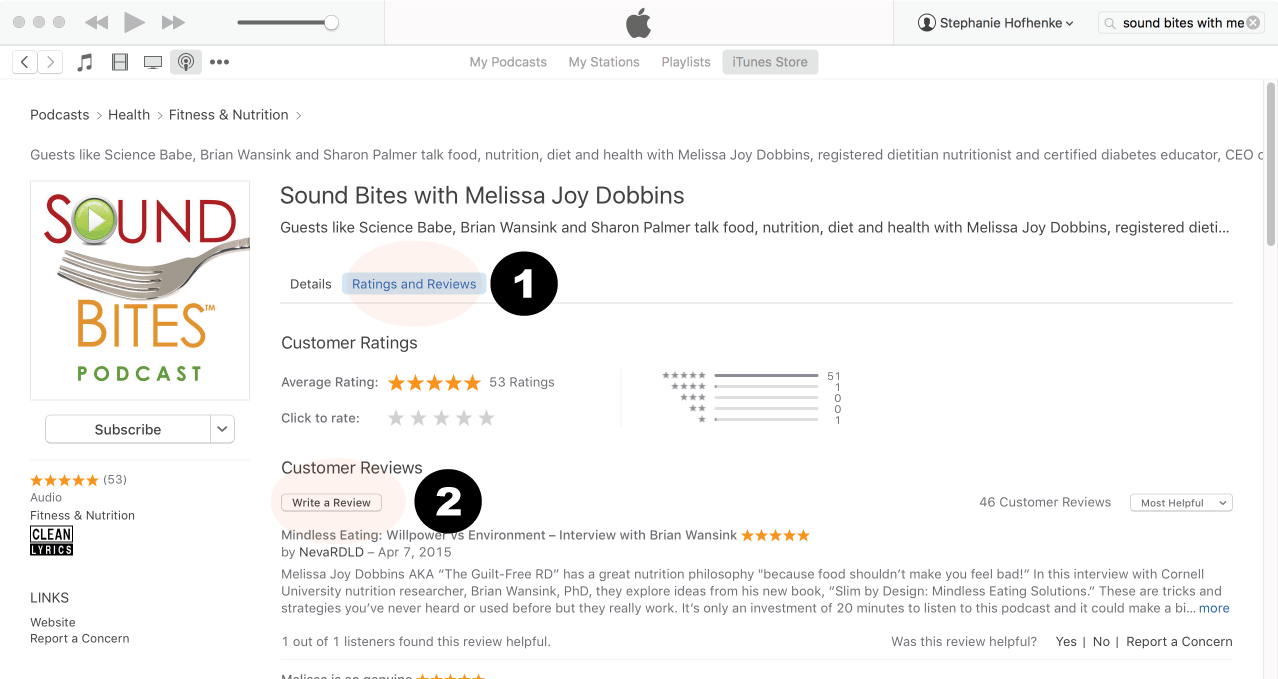
Click Ratings & Reivews
Click Write a Review
View reviews and write your own review.
Write your review…. Thank you!
Write your review!
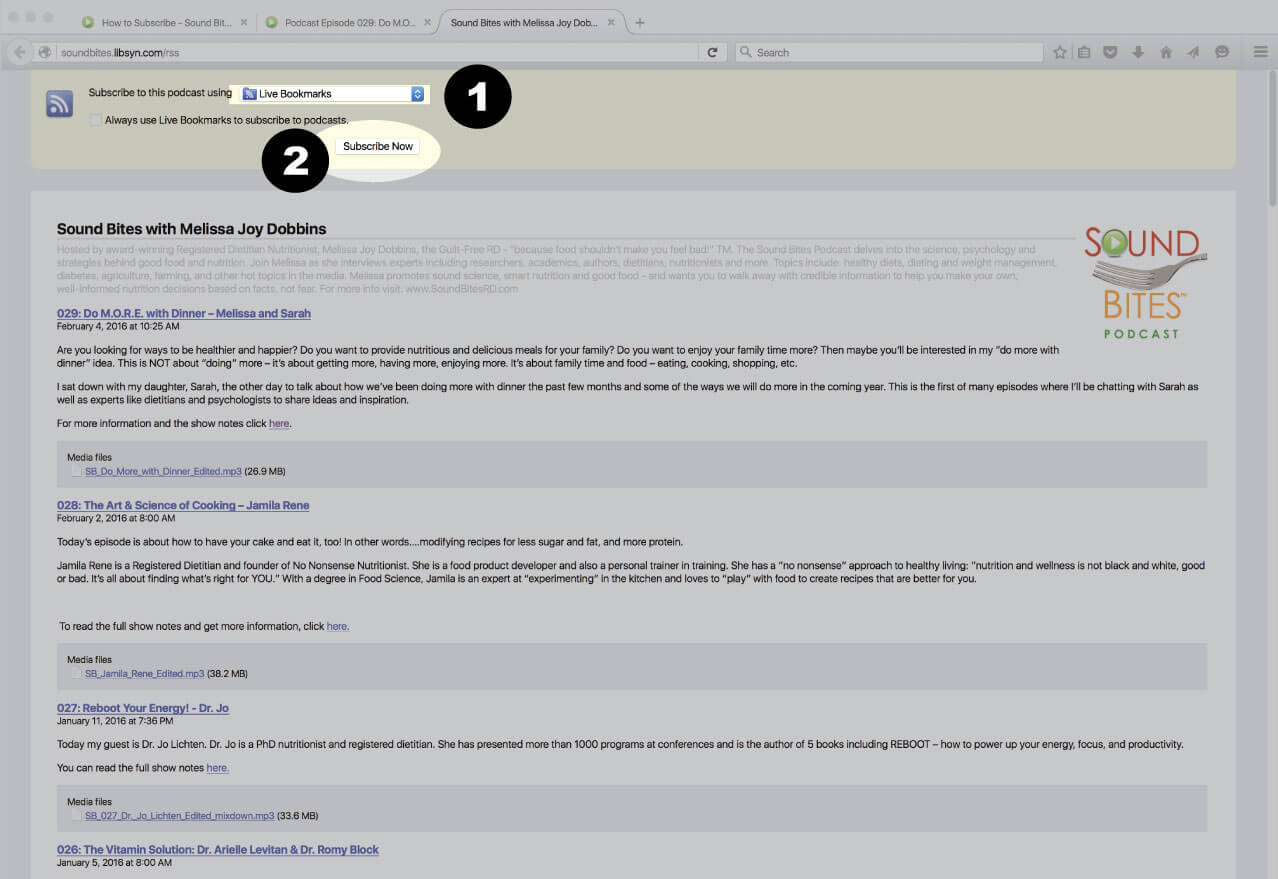
Subscribe via RSS Feed
Navigate to any podcast player . Click on the RSS feed icon.
Click on the RSS feed icon.
Click on RSS Feed
Choose which application you would like to use to receive the RSS feed
Click “Subscribe Now”
Confirm settings and subscribe.
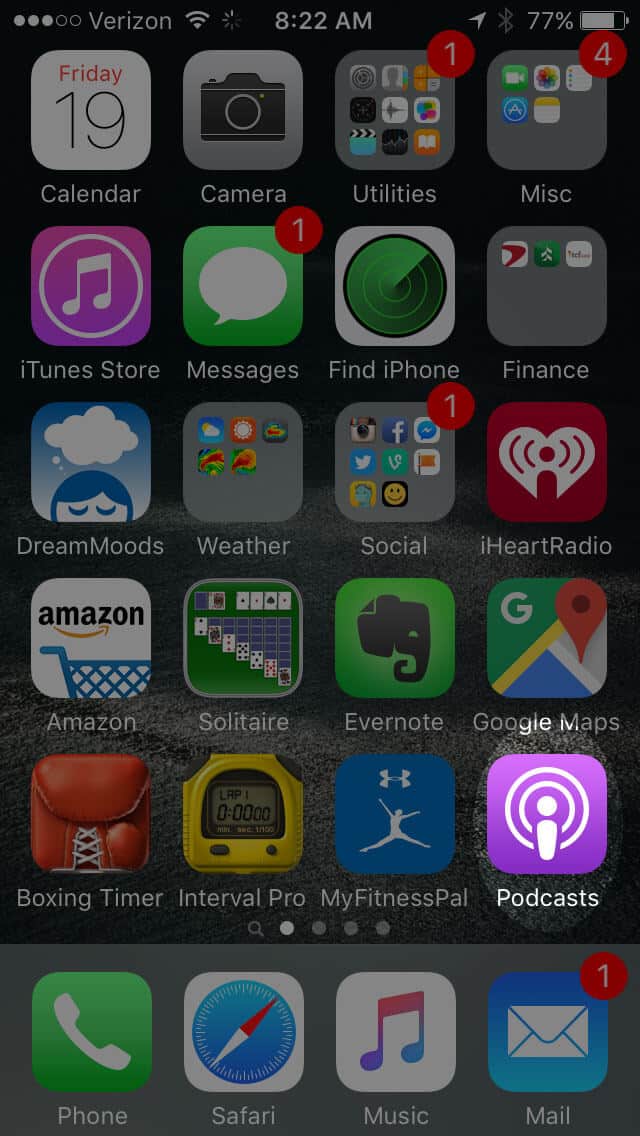
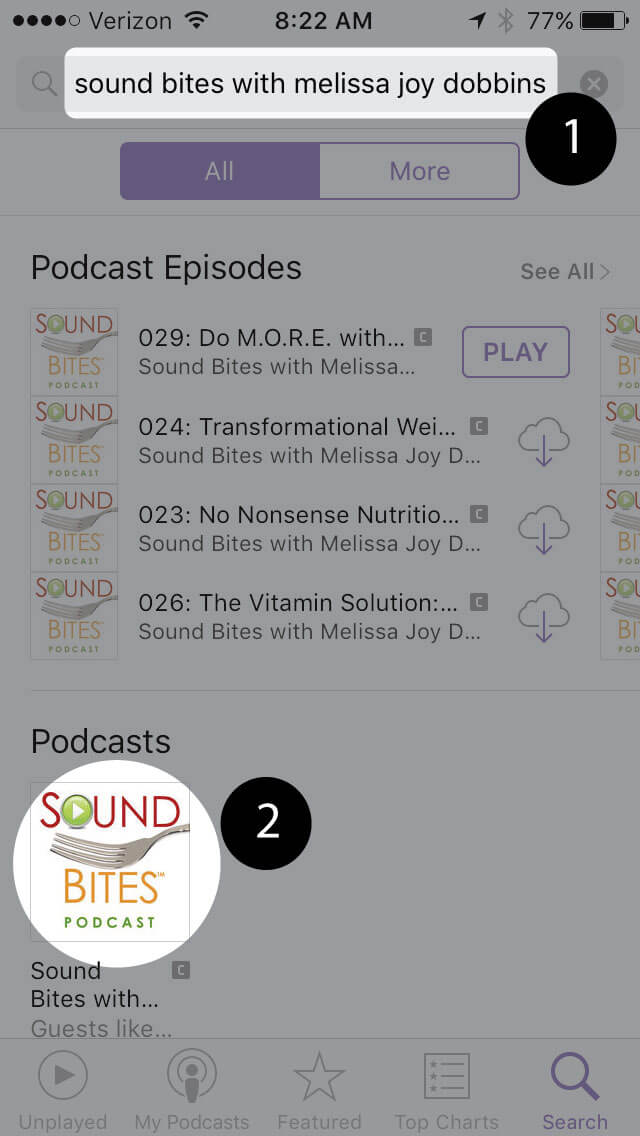
Subscribe & Review on iPhone
Open the “Podcast” app on your iPhone
Search for “Sound bites with melissa joy dobbins”
Open the podcast and click “Subscribe” and your done!














Great content
Glad there was mention of Eating Disorders
Thanks Deborah – glad you enjoyed it!
Melissa